13-23% of people experience psychotic symptoms at some point in their lifetime resulting from a number of organic causes (Perala, 2007; van Os, 2001).
“we cannot make the diagnosis if it’s not on our differential”
13-23% of people experience psychotic symptoms at some point in their lifetime resulting from a number of organic causes (Perala, 2007; van Os, 2001).
“we cannot make the diagnosis if it’s not on our differential”
The presence of the following are more consistent with an organic cause of psychosis (Sheitman, 1997):
Presence of any one of the following 4 factors that favor organic vs. functional psychosis can be used as triage method (Dubin, 1983):
[D] - Drugs / Toxins
[I] - Infective
[V] - Vascular
[I] - Inflammatory
[N] - Nutritional
[E] - Endocrine
[M] - Metabolic
[D] - Degenrative
[T] - Trauma
[T] - Tumor
[S] - Seizure
Geriatric population, multiple comorbidities, Anticholinergic cognitive burden scale, Another calculator.
Psychiatric symptoms often develop after 4 days of corticosteroid therapy, although they can occur late in therapy or after treatment ends. Delirium often resolves within a few days, psychosis within 7 days, and mania within 2 to 3 weeks, whereas depression can last for more than 3 weeks.
| Grade | Symptoms |
| 1 | Mild, nonpathologic, and subclinical euphoria |
| 2 | Reversible acute or subacute mania and/or depression |
| 3 | Bipolar disorder with relapses possible without steroids |
A 3-level grading system can gauge severity of corticosteroid-induced psychosis; grade 2 or 3 warrants treatment
Central Anticholinergic Effects

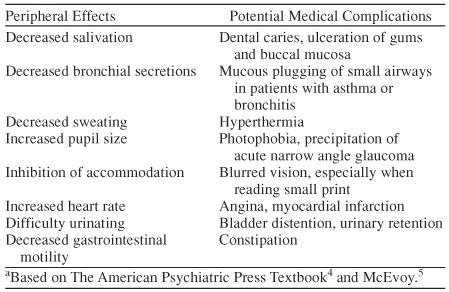
Peripheral Anticholinergic Effects
Check pockets for sharps and needles!
Acute: agitation, paranoia, hallucinations, hyperthermia. Chronic: cognitive impairment, suicidal ideation or attempt
Symptoms : AMS, seizures, restlessness, hyperthermia, ataxia, halos; palpitation, chest pain; GI complaints; Piloerection; Bruxism. May also present with serotonin syndrome.
Alcohol withdrawal symptoms appear within 6-24 hours after stopping alcohol, are most severe after 36 – 72 hours and last for 2 – 10 days.
Symptoms include: Anxiety, sweating, tremors, increase HR and BP, insomnia, nausea and vomiting, diarrhea
Severe withdrawal involve: Seizures, Hallucinations, Delirium tremens, Extreme fluctuations in body temperature and blood pressure, Extreme agitation
Alcohol withdrawal scale [CIWA-Ar]
| CIWA-Ar score | Interpretation (Withdrawal severity) |
| 0 – 9 | Absent or minimal |
| 10 – 15 | Mild |
| 16 – 20 | Moderate |
| 21 – 67 | Severe |
Symptoms include: Anxiety, Insomnia, Restlessness, Agitation and irritability, Poor concentration and memory, Muscle tension and aches
Short-acting benzodiazepines include oxazepam, alprazolam and temazepam. Withdrawal typically begins 1-2 days after the last dose, and continues for 2-4 weeks or longer.
Long-acting benzodiazepines include diazepam and nitrazepam. Withdrawal typically begins 2-7 days after the last dose, and continues for 2-8 weeks or longer
No monitoring scale is recommended as symptoms can fluctuate markedly, rather reassess patient every 3-4 hrs.
Calculating diazepam equivalent doses
Low-dose benzodiazepine reducing schedule
High-dose benzodiazepine reducing schedule
Short-acting opioids (e.g. heroin): Onset 8-24 hours after last use; duration 4-10 days.
Long-acting opioids (e.g. methadone): Onset 12-48 hours after last use; duration 10-20 days.
| Symptom | Not present | Mild | Moderate | Severe |
|---|---|---|---|---|
| Feeling sick | 0 | 1 | 2 | 3 |
| Stomach cramps | 0 | 1 | 2 | 3 |
| Muscle spasms or twitching | 0 | 1 | 2 | 3 |
| Feeling cold | 0 | 1 | 2 | 3 |
| Heart pounding | 0 | 1 | 2 | 3 |
| Muscular tension | 0 | 1 | 2 | 3 |
| Aches and pains | 0 | 1 | 2 | 3 |
| Yawning | 0 | 1 | 2 | 3 |
| Runny/watery eyes | 0 | 1 | 2 | 3 |
| Difficulty sleeping | 0 | 1 | 2 | 3 |
| Score | Suggested withdrawal management |
|---|---|
| 0-10 | Mild withdrawal; symptomatic medication only |
| 10-20 | Moderate withdrawal; symptomatic or opioid medication |
| 20-30 | Severe withdrawal; opioid medication |
Dysuria, Urinary frequency, Hematuria. Other sx - Urinary urgency, Suprapubic Pain more
Headache, Nuchal rigitity, Fever, Nausea, Vomiting, Altered LOC, Focal deficits, Seizures. more
Temperature [Fever, Hypothermia(<36)]
Hypotension SBP <90, SBP drop >40, MAP <65
Cold clammy skin
Tachycardia
Low O2 level
Additional = High WBC; Incr ESR, CRP, PCT;
This page was last updated on 26/11/18.