Many cause fatigue and depression. Depression associated with beta-blockers, reserpine, and methyldopa
Although beta-blockers (especially propranolol and metoprolol) were thought to cause depression, recent studies and meta-analyses show that they do not
Used in pregnancy-induced hypertension (HTN). Causes sedation, fatigue and depression, mostly with prior history of depression. Causes norepinephrine depletion
Causes depletion of cathecholamines, leading to sedation, malaise, fatigue. May be associated with depression, but unclear
Calcium-channel blocker, secondary agent for migraine prophylaxis. In a trial, 8% of patients treated prophylactically developed depression. Also causes extrapyramidal side effects (EPS)
Epilepsy increases depression risk, but some anticonvulsants are associated with additionally increased risk
Work on the Gamma-Aminobutyric (GABA) system and may produce fatigue, sedation, impaired cognition, and depressed mood
Clinically associated with neuropsychiatric side effects, e.g. in one study, 8% had intolerable neuropsychiatric side effects, including aggression, irritability, mood swings, and depression
Increases CNS GABA levels. Trials found a 12% versus 3.5% prevalence of depression in vigabatrin- versus placebo-treated patients
Linked to new depression in 10% of patients. Usually in patients with personal or family history and with rapid dose escalation
Classical symptoms - nystagmus, ataxia, nauseas and vomiting. Case report of 2 patients presenting with vegetative symptoms of depression without classical symptoms of toxicity. ression in 10% of patients. Usually in patients with personal or family history and with rapid dose escalation
phenobarbital may cause depression associated with suicidal ideation
In infected, medically ill patients, cytokine-driven sickness behavior, psychological reaction, delirium, and medication side effects must be differentiated
Indicated for bacterial infections, acne, chlamydial infections, Helicobacter pylori; side effects are photosensitivity, lupus-like, gastrointestinal (GI) side effects
Side effects include ototoxicity, dysfunction of the optic nerve (scotomas), and renal toxicity
Used for respiratory and skin infections. May cause hepatotoxicity, GI distress, QTc prolongation
NNRTI, used in HIV. May cause vivid dreams, anxiety, depression. Symptoms transient in most and dose-related
Used in the treatment of severe acne. 24 reports of depression and more than 170 cases of isotretinoin-associated suicide have been reported.
May be used for treatment of hepatitis C virus infection or melanoma. Induces depressive symptoms in up to 58% of patients
Neurologic, rheumatologic, GI, respiratory, oncologic illnesses. Symptoms may vary from subtle anxiety/depression to full-blown affective and psychotic syndromes. Dose-dependent.
Depressive symptoms may occur after initial corticosteroid administration, with long-term use, or with drug discontinuation
Immunosuppression in transplant patients, RA, psoriasis; side effects include hypertension, nephrotoxicity
Used in Parkinson's disease (PD). Associated with depression in small percentage of patients
Associated with depression in small percentage of PD patients, but has also been shown to help depression as an adjunct in PD patients
Benzodiazepines-reports and small studies report association with depression and even suicide. Associated with higher doses and lower anxiety
Some reports suggesting association with depression. Also causes EPS, such as parkinsonism
In overdose lead to vasodilatation, anhydrosis, hyperthermia, delirium, and urinary retention
Side effects include hepatotoxicity, rash, CNS dysfunction including drowsiness and lethargy, restlessness, disorientation, headache, etc.
Side effects include extrapyramidal reactions, such as tardive dyskinesia cardiovascular, endocrine, and skin reactions
Patients with pre-existing psychiatric illness may experience worsening of symptoms
Antimitotic agent: side effects include marrow suppression, neurologic (paresthesias) GI, SIADH, cardiovascular
Antimitotic agent: side effects include marrow suppression, pulmonary, and neurologic
Some studies suggest link with depression, but well-designed large studies are lacking. Associated with progestins
Undulant fever - a bacterial zoonosis transmitted to humans from infected animals: septic arthritis, neurologic involvement. more
Fever, night sweats, weight loss, fatigue, loss of appetite, cough and hemoptysis. more
Primary - chancre. Secondary: rash including palms and soles, fever, meningitis. Late: gummas, neurosyphilis, cardiovascular. more
History of tick bite, erythema migrans, and neurologic findings with constitutional complaints. more
Relapsing fevers, anxiety, psychosis, combative and excitable behaviors, confusion, delirium, depression, catatonia, stupor, coma, decerebrate posturing, death. more
Tapeworm (Taenia Solium) infection of the brain. Ingestion of eggs from pork, infected vegetables. Seizures, headache, parkinsonism, obstructive hydrocephalus, CN palsy, maybe skeletal muscle lesion or visual loss. more
Toxoplasma gondii from infected cat feces. Immunocompetent patient - mild flu like symptoms 1-2 weeks. Immunocompromised patient - encephalitis, cognitive impairment, focal neuro deficit. more
Insidious onset, irregular fever, cough, anxiety, irritability, lethargy, coma. more
Prior history of infection with stupor, coma or nuchal rigidity. Excessive sleeping afterwards. Irritability and anger.
Limited attention span. Typical depressive thought content not marked. more
Tropheryma whippelii infection. Rare disease that commonly starts with GI complaints, but because of multisystem involvement, presentation can be quite variable. May go undected for years. Pt may present with sx other than GI. more
Systemic sx
Wt loss, diarrhea, occult blood loss, jt pain, non specific abdo or chest pain, fever, glossitis and abdo fullness
CNS sx
Fewer than 10-15% of patients with Whipple disease eventually develop clinically significant CNS involvement. A review of patients with CNS-WD showed that by the time of CNS disease onset they often report previous systemic problems
Fewer than 100 cases of patients with confirmed CNS-WD have been reported.
Almost 50% of these patients had a concomitant psychiatric illness (eg, depression, hypomania, anxiety, psychosis; mostly with delusional content, or change in personality).
Two thirds of patients with altered mentation (almost 50% of all patients with CNS-WD) had dementia.
Hypothalamus-related problems (eg, polydipsia, hyperphagia, decreased libido, amenorrhea, change in sleep-wake cycle with insomnia
myoclonus, opthalmoplegia, seizures
Sudden onset of persistent motor or sensory dysfunction. more
"Based on pooled data, the overall prevalence [post-stroke] of major depression was 21.7% and minor depression was 19.5%." Post stroke depression: a review
Physical and cognitive impairment with a step-wise progression. hypertension is frequent. more
In a study by Cummings et al, while 17% patients with DAT had depressive symptoms, 60% of patients with MID had depressive symptoms. more
Basically any disorder that causes Hypoxemia. causes of hypoxemia
a) Environmental O2 insuff; high altitude sickness
b) Pulmonary disease -> poor oxygenation of blood;
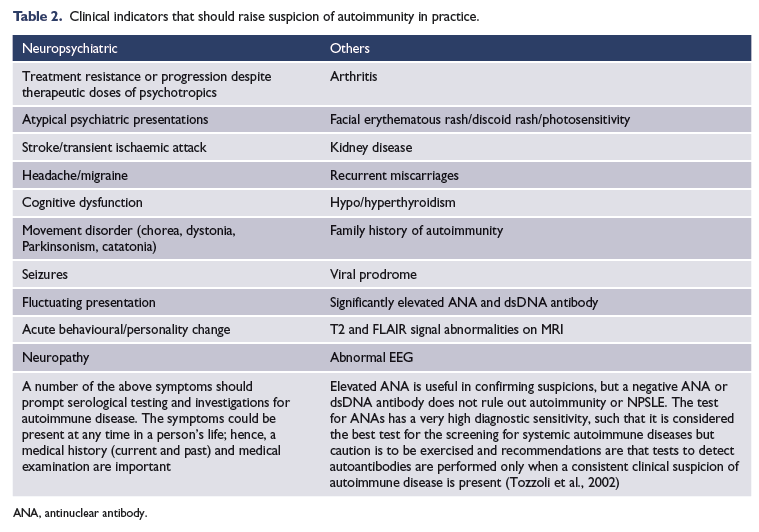
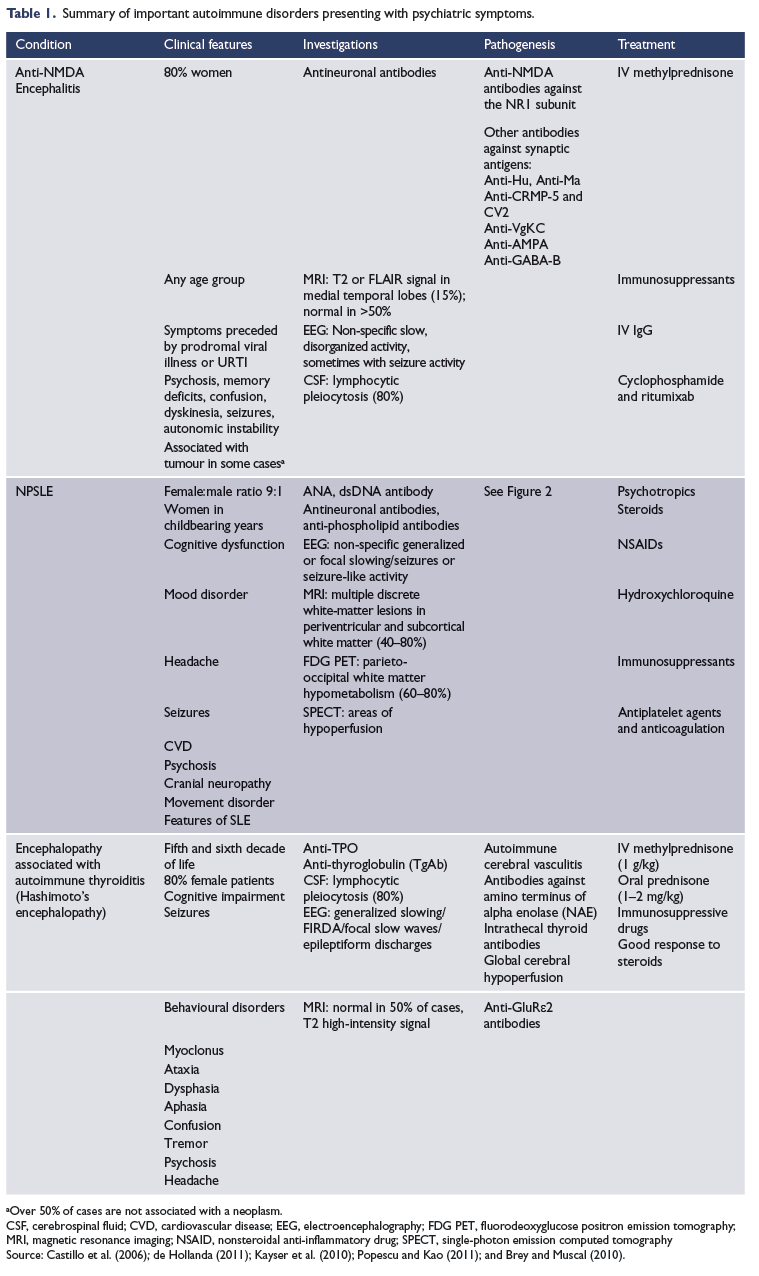
"Psychotic manic-like and depressive-like episodes may be the initial presentation of Connective Tissue Disorders. Screening of ANA and anti-DNAds may warranted if clinically suspected."
Symptoms include anorexia, weight loss, myalgia; rheumatoid nodules and small joint deformities, and pain; vasculitis, pericarditis; pleural effusions, pulmonary fibrosis; spinal cord compression, peripheral neuropathy; neuropsychiatric disorders.more
90% are women, more common in Asians and blacks. Photosensitivity, discoid or malar rash, oral ulcers; fatigue, weight loss, fevers; arthralgias and arthritis; pleuritis, pericarditis; renal disease; anemia, leucopenia. more
Widespread pain (typically in all four body quadrants) for at least 3 months and tenderness at 11+ of 18 specific sites on the body. more
Aching and morning stiffness in shoulders, hip girdle, and neck, typically in patients over 50. Also fever, malaise, fatigue, weight loss.more
Classic celiac disease present with signs and symptoms of malabsorption, including diarrhea, steatorrhea, iron-deficiency anemia, and weight loss or growth failure
Nonclassic celiac disease, patients may present with nonspecific gastrointestinal symptoms without signs of malabsorption, or with extraintestinal manifestations (without gastrointestinal symptoms). patients mainly presenting with unexplained iron-deficiency anemia.
Asymptomatic celiac disease - Many patients, especially those diagnosed during screening, report no symptoms even on detailed questioning, and despite the presence of characteristic intestinal lesions. A gluten-free diet often leads to improvement in the quality of life, even in patients who considered themselves asymptomatic at the time of diagnosis. more,
symptoms
Morning stifness, oral and genital ulcers. Skin rashes, Joint pain, Neurologic changes. more
"Some of the psychiatric Behçet patients have relatively acute onset symptoms and can be evaluated within the scope of organic confusional disorder."
"Additionally, many Behçet patients present with chronic psychiatric problems in the absence or presence of accompanying neurological symptoms. Anxiety and depression are frequently encountered in these patients and might occasionally precede the onset of the disease."
9/10 women, middle aged. Most common [93-98% pts at presentation] - dry eyes or dry mouth. more, case report
other associations - GI symptoms, renal conditions, lymphadenopathy, arthritis, bronchitis, vasculitis, fever, fatigue
In a cross-sectional study of primary Sjogren patients - "33.8% patients had anxiety, and 36.9% had depression" link
Can affect all organ systems. Asymptomatic initially in many patients - often diagnosed as Hilar Adenopathy on CXR. Pulmonary presentation [45%] with cough, dyspnea and non-specfic chest pain. Constutional presentation [25%] with fever, wt loss, fatigue and malaise. more
Psych manifestations reported in 5-20% patients. Case reports of neurosarcoidosis preseting as pseudodementia, depresssion, non-specific somatic c/o
Includes suspected SLE, Systemic Sclerosis, Poly/Dermatomyositis/Sjorgens/Mixed connective tissue disease. Consider referral if multiple of the following symptoms:
Joint pain - pattern is distinctive; upper and lower extremeties tend to be symmetrically affected; Distal > Proximal; Thoracic and Lumbar spine are usually spared.
Morning stiffness is usually present, but not specific. Swan-neck and ulnar subluxation are not disease-specific changes, although they are often considered rheumatoid deformities. SLE or Scleroderma pts may have
joint complaints at all.
Skin changes - Malar rash,discoid lesions, photosensitivity, alopecia, mucous membrane ulcers, skin thickening, telangiectasia, and purpura or ulcers from vasculitis may be present.
If the answer to both the following questions is negative, the presence of Raynaud's phenomenon is unlikely. "Do you have any circulation problems?" -> "Do your fingers turn white or blue in the cold?"
Chest discomfort - Serositis or esophageal dysmotility with reflux may cause chest discomfort. Defining symptom of pleurisy is a sudden sharp, stabbing, burning or dull pain in the right or left side of the chest during breathing, especially when one inhales and exhales.
Pericarditis typically presents with acute onset severe, sharp retrosternal chest pain, often radiating to the neck, shoulders, or back. Positional changes are characteristic with worsening of the pain in the supine position and with inspiration; and improvement with sitting upright and leaning forward.
Esophageal disease initially presents with heartburn and later dysphagia.
Other sx
Anaemia, Thrombocytopenia, lymphopenia
Foamy urine may indicate protienuria; hematuria
Dry eyes / dry mouth
Work-up
CBC, ESR, CRP, Creat, LFT
Urine R/M
CXR if possible polymyositis/or Respiratory system involvement
ANA, Complements, CK [for polymyositis] - in consultation with experts
Acute or subacute mood/behavioral changes, short-term memory problems, complex-partial seizures, cognitive dysfunction. Also hyperthermia, somnolence, and endocrine abnormalities. Most common associated malignancies - lung (small cell carcinoma; SCC), testicular, breast, ovarian, thymoma, Hodgkin lymphoma. Or there may be no malignancy [i.e. non-neoplastic]. more, cases
Depressive symptoms are associated with anemia in a general population of older persons living in the community
Common with certain anticonvulsants (e.g. valproic acid), elderly, alcoholics, eating disorders, malnourished. Symptoms include cognitive dysfunction. Signs - megaloblastic anemia. more
Megaloblastic anemia, myelopathy (subacute combined degeneration), dementia, delirium, peripheral neuropathy. Occurs in pernicious anemia, chronic peptic ulcer disease, after gastrectomy or gastric bypass, alcohol dependence, irritable bowel disorder, eating disorders, malnourished. more
Peripheral neuropathy, seizures, migraines, chronic pain, depression, psychosis. Elevated homocysteine. Many drugs act as antagonists of B6. more
Pellagra: pigmented rash of sun-exposed areas, bright red tongue, diarrhea, apathy, memory loss, disorientation. more
Weakness, fatigue, somnolence, cold intolerance, weight gain, constipation, hair loss, hoarseness, stiffness, muscle aches, bradycardia, facial puffiness, slowed speech. more
Symptoms include nervousness, anxiety, irritability, sweating, fatigue, heat intolerance, weight loss, muscle weakness. Signs include arrhythmias, e.g. atrial fibrillation, myxedema, proptosis. more
Increased thirst, frequent urination. Complications include cardiovascular disease, retinopathy, nephropathy, peripheral and autonomic neuropathy. more
Paresthesias, muscle cramps, carpopedal spasm, rarely facial grimacing, severe - tetany and seizures. more
Anemia, anorexia, nausea, vomiting, diarrhea, abdominal pain, weight loss, muscle weakness. In Addison's disease, increased ACTH causes hyperpigmentation, especially in sun-exposed skin, scars, mucous membranes. Postural hypotension due to low mineralocorticoids; hypoglycemia when stressed or fasting; hyponatremia, hyperkalemia. more
Truncal obesity and striae, diabetes, hypertension, hyperglycemia, muscle weakness, osteopenia, skin atrophy and bruising, increased susceptibility to infections, gonadal dysfunction. Due to use of corticosteroids, excessive ACTH secretion (if by a pituitary tumor, called Cushing's disease), and adrenal tumors. more
Mood symptoms present during the week prior to menses, resolving within a few days after menses starts. Might be accompanied by breast tenderness, muscle aches, abdominal bloating, and weight gain. more
Typical onset is at 51 years. Symptoms include hot flashes, night sweats, palpitations, dizziness, fatigue, headaches, joint pains. more
Amenorrhea or oligomenorrhea, infrequent or absent ovulation, increased levels of testosterone, infertility, truncal obesity or weight gain, alopecia, hirsutism, acanthosis nigricans, hypertension, insulin resistance. more
Increase in rate and depth of breathing for a few minutes leading to dizziness or syncope due to respiratory alkalosis. Also might have carpopedal spasm, myoclonic jerks, paresthesias. more
Multi-system dysfunction, lethargy, altered mental status, seizures. more
Stages 0 [minimial hepatic enceph] and Stage 1 are likely to mimic depression. Beyond that astrexis is obvious. more 1, more 2.
Severe Disease - Stupor, Coma, Dementia, Extrapyramidal signs, Fetor hepaticus (Odor of breath from mercaptans)
Stage 0. MHE (previously known as subclinical HE). Symptoms relate to disturbances in sleep, memory, attention, concentration and other areas of cognition. A classic sign of HE is a sleep disturbance. Asterixis is absent.
Stage 1. Trivial lack of awareness. Shortened attention span. Impaired addition or subtraction. Hypersomnia, insomnia, or inversion of sleep pattern. Euphoria, depression, or irritability. Mild confusion. Slowing of ability to perform mental tasks. Asterixis can be detected.
Stage 2. Lethargy or apathy. Minimal disorientation. Inappropriate behavior. Slurred speech. Obvious asterixis. Drowsiness, lethargy, gross deficits in ability to perform mental tasks, obvious personality changes, inappropriate behavior, and intermittent disorientation, usually regarding time.
Stage 3. Somnolent but can be aroused, unable to perform mental tasks, gross disorientation about time and place, marked confusion, amnesia, occasional fits of rage, present but incomprehensible speech.
Stage 4. Coma with or without response to painful stimuli. However, the terms that limit each stage of the classification are not clearly defined, and the metric characteristics of the stage are unknown. It is for this reason that other scales such as the Clinical Hepatic Encephalopathy Staging Scale (CHESS) have been proposed.16 The presence or absence of the nine items on the CHESS score may be helpful in eliminating interobserver variability and in making a distinction between the various grades of encephalopathy. This staging scale, however, requires further validation.
Higher risks for dementia in dialysis patients. Need regular dementia work-up. Might have higher risk for vascular dementia, but also associated with uremia. Aluminum toxicity now less common. more, Dialysis disequilibrium syndrome
Abdominal pain, peripheral neuropathy, and mental disturbances. Seizures, autonomic instability, dehydration, electrolyte disturbances, dermatologic changes also may occur. Physical symptoms occur in attacks, but psychological ones may persist. more, more detailed
Onset in childhood and adolescence, but can occur as late as fifth decade. Symptoms include personality and behavioral disturbances, dementia, EPS, dysarthria, liver cirrhosis. Almost all have Kayser-Fleischer rings. more
Multiple episodes; acute onset involving muscle weakness, monocular blindness, vertigo, bladder dysfunction, and incoordination. more
Tremor, bradykinesia, gait disorder, and rigidity. more
Younger age of onset (e.g. 53) than Alzheimer's disease, with prominent lability, distractibility, decrease in insight, and personality changes. more, criteria
Choreoform movements, ocular dysfunction, dementia, and frequent depression with 10% psychosis. more
Uneven cognitive decline, language and visual specific dysfunction. more
Mild extrapyramidal symptoms, sudden changes in cognition, visual hallucinations, rapid eye movement sleep disorder. more
Cognitive decline associated with signs of cortical injury, e.g. aphasia, apraxia, etc. more
Acute global disturbance of cortical functioning that causes fluctuating level of attention, consciousness, cognition, and perception. more
More salient apathy, slowed mentation, and gait dysfunction. more
Supranuclear gaze palsy, especially in vertical direction, truncal rigidity, akinesia, postural instability, early falls, dysarthria, dysphagia; subcortical dementia; pseudobulbar affect. more
Combination of upper motor (weakness, hyperreflexia, spasticity) and lower motor neuron (atrophy, fasciculations) signs. Presents with asymmetric limb weakness (80%) or bulbar disorders of dysphagia or dysarthria (20%). Might be accompanied by pseudobulbar affect, cognitive impairment, autonomic symptoms, parkinsonism, supranuclear gaze paresis, sensory loss. more
Traumatic brain injury associated with headaches, cognitive dysfunction, dizziness, and neuropsychiatric symptoms. more
"Twenty-two percent of the sample reported minor depression, and 26% reported major depression at 1-year post-TBI." [n=1570] link
Amongst hospitalized patients with TBI, depression rate at 1 year was 53%. [n=599] link
Higher depression scale score at 1 week, older age and abonormal CT scan predicts depression at 3-months in Mild TBI patients. link
History of trauma: unilateral headache and pupillary enlargement, and stupor, coma, and hemiparesis if large. more
"Pooled mean prevalence of depression in cancer patients ranged from 8% to 24%" link. "Depression is highly associated with oropharyngeal (22%-57%), pancreatic (33%-50%), breast (1.5%-46%), and lung (11%-44%) cancers. link.
Headaches-classic "early morning" nausea/vomiting, seizures, syncope, neurologic deficits. more, causes of SOL
Cough, hemoptysis, chest pain, dyspnea, hoarseness. Associated with smoking. more
Abdominal pain and weight loss out of proportion to the degree of psychological symptoms. Anorexia, early satiety, back pain in more progressive disease. Diabetes might also be present. more
Acute or subacute mood/behavioral changes, short-term memory problems, complex-partial seizures, cognitive dysfunction. Also hyperthermia, somnolence, and endocrine abnormalities. Most common associated malignancies - lung (small cell carcinoma; SCC), testicular, breast, ovarian, thymoma, Hodgkin lymphoma. Or there may be no malignancy [i.e. non-neoplastic]. more, cases
Repeated seizures without a causative factor. Seizures may be followed by a post-ictal period of depression or psychosis.more
"Symptoms of depression are overrepresented in INPH patients compared with the population, despite treatment with a shunt. Screening for depression should be done in the evaluation of INPH patients in order to find and treat a coexisting depression." link
Snoring, daytime sleepiness, awakening with sensation of choking, gasping; restless sleep, nocturia, morning headaches, episodes of breathing cessation, hypertension. more
Chronic daytime sleepiness with episodic sleep attacks; also cataplexy, sleep paralysis, hypnagogic and hypnopompic hallucinations. more
Patients are obese and most have co-existing obstructive sleep apnea (OSA). Many also have pulmonary hypertension with right-sided heart failure. Dyspnea on exertion distinguishes from pure OSA. more
Subjective discomfort of lower extremities and need to move, worse at night. Most idiopathic, but may be associated with iron deficiency, uremia, diabetes, rheumatic disease, venous insufficiency. more
Motor (simple or complex) and vocal tics (sounds or actual words). Starts in childhood. more
Mental retardation, in association with non-neurologic physical abnormalities. more
Tay-Sachs disease (in Ashkenazi Jews) - adult form: clumsiness in childhood, progressive weakness later, followed by motor dysfunction and intellectual decline. more
Cerebellar ataxia, pyramidal signs, and intellectual dysfunction. more
Syndrome of prolonged headaches lasting 4 hours or longer. Encompasses constant (transformed) migraines, chronic tension-type headache, medication overuse headache, hemicrania continua, and new daily persistent headache. more
Disorder of a body region, usually of the extremities, characterized by pain, swelling, limited range of motion, vasomotor instability, skin changes, and patchy bone demineralization. Frequently begins following an inciting event. more
Depressed mood for two weeks or more, and a loss of interest or pleasure in everyday activities, accompanied by other symptoms such as feelings of emptiness, hopelessness, anxiety, worthlessness, guilt and/or irritability, changes in appetite, problems concentrating, remembering details or making decisions, and thoughts of or attempts at suicide. more
At least 2 years of depressed mood; may co-exist with MDD. more
Affective lability, depression and/or anxiety as well as neurovegetative symptoms present in the majority of menstrual cycles in the final week before the onset of menses, improving within a few days after the onset of menses, and resolved within a week after menses. more
Emotional response to a stressful event, such as onset of illness, divorce, financial problems. Symptoms start within 3 months of the stressor and remit within 6 months of stressor removal. more
Presence of one or more somatic symptoms that are distressing or result in significant disruption of daily life with excessive thoughts, feelings, or behaviors related to these somatic symptoms. more
Excessive and uncontrollable worry about a number of anxiety-provoking events. more
Characterized by psychotic symptoms as well as presence of manic or depressed episode; psychotic symptoms must exist outside the mood symptoms for at least 2 weeks. more
Dominated by psychotic symptoms of hallucinations, delusions, disorganized thought process, speech, behavior, negative symptoms. Onset typically teens to early 20s in males and late 20s in females. more
In Bipolar I, there must be at least one manic episode. In Bipolar II, there must be presence of hypomanic AND depressive episodes. more, Unipolar v/s bipolar depression
Attenuated bipolar disorder, frequently starts before age 21; frequent short cycles of subsyndromal depression and hypomania, not meeting criteria for bipolar disorder. more
Extreme agitation, delirium, confusion, sleeplessness, hallucinations, delusions with onset usually 3-14 days postpartum. Increased risk for suicide and infanticide
Trauma-associated flashbacks, nightmares, avoidance, hyper-vigilance, and sleep disturbance. more
Poor concentration, attention and memory, difficulties with task completion. more
Demoralized - difficulty in coping with medical illness
Close temporal association with illness. Few neurovegetative symptoms. Able to maintain future orientation/hope
-Compassion, recognition, and normalization. -illness-specific supports (groups, social work, chaplaincy) -Physical therapy (eg, PT/OT).
Occurs in response to a significant loss, such as death of loved one. In addition to depressed mood, also have sympathetic arousal and restlessness. Criteria for Major Depressive Episode not met. more
Disaffiliated - grief
Few neurovegetative symptoms. Able to maintain future orientation/hope. Improvement typical as time since loss increases
-Supportive therapy
-Spiritual support
“Difficult” - patients have a breakdown in the therapeutic alliance with their treatment team
Mood changes often intense, immediate, and reactive to situation. Frequent breakdowns in communication with care team. Care team more distressed by patient’s symptoms than the patient
-Frequent communication among care team members
-Multidisciplinary care conferences to clarify salient issues
-Provide patients with consistent information and expectations
{kind=link}